Out-of-staters are flocking to places where abortions are easier to get
By Mallika Seshadri
On April 16, 2023
WASHINGTON, D.C. (NPR) — When Mara Pliskin started working at Planned Parenthood Illinois, she didn’t expect to feel like a travel agent.
Now, the abortion navigation program manager and her co-workers joke that that’s half the job — booking flight, train and bus tickets for out-of-state abortion seekers, arranging hotel stays and giving them money for food and gas.
“We’re being as creative as possible to really just work with every individual patient to resolve all those barriers that might stand in the way between making their decision and getting to our door,” she said.
What Pliskin and her colleagues face isn’t unusual.
Even before Roe v. Wade was overturned last June, almost 10% of patients seeking abortions traveled out of state. But since the Supreme Court’s decision, providers in some so-called “sanctuary” states where abortion access is protected are seeing record high out-of-state demand.
In Colorado, preliminary numbers show more than twice as many people from other states came for an abortion in 2022 compared to 2021.
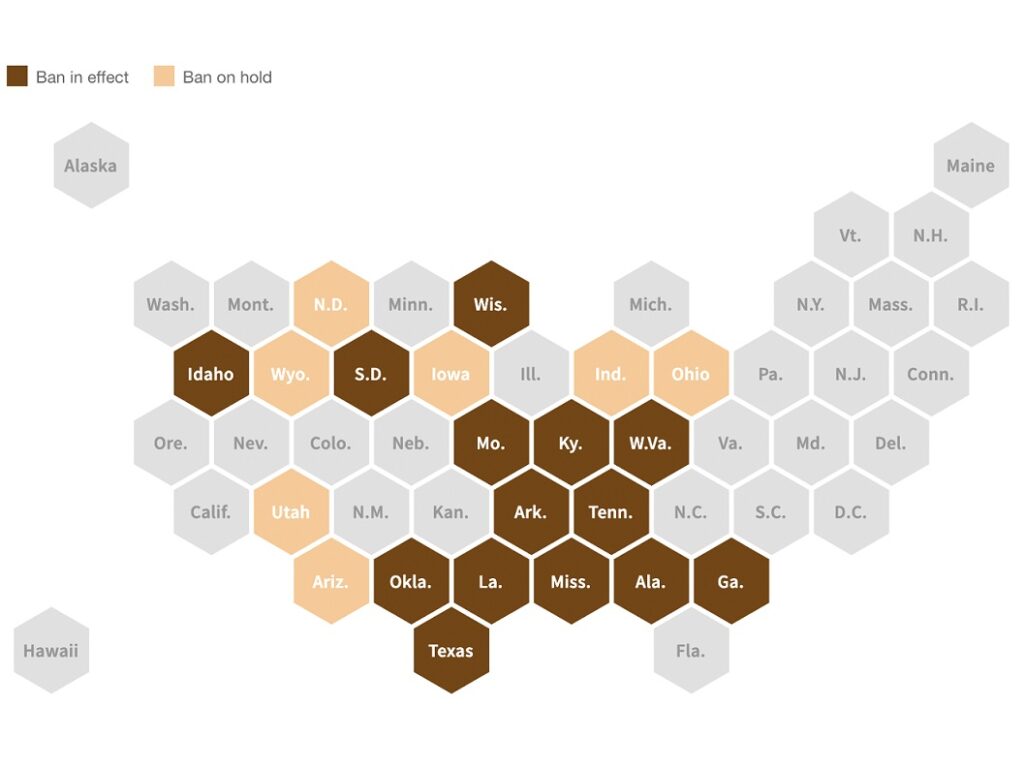
While about a quarter of the states have restricted or banned abortions since the Supreme Court’s decision, more than 25, including Colorado, have taken steps to do the opposite. Many of those states are clustered in the Northeast and on the West Coast.
creased demand in “sanctuary states”
Illinois is surrounded on all sides by states categorized as “restrictive” or “most restrictive” by the The Guttmacher Institute. And after Roe v. Wade was overturned last June, the state has administered an average 1,140 more abortions each month, according to a #WeCount report released by the Society of Family Planning.
In some Illinois clinics, out-of-state abortions have risen six-fold, from roughly 5% to about 30%, since the Supreme Court’s decision.
The majority are from neighboring states with restrictions, like Wisconsin, Pliskin said. But a number are coming from Kentucky, Tennessee, Missouri, and southern states as far as Louisiana, Mississippi, Alabama and Florida.
Thirty-five states have been represented where she works.
“As a person with birthing capacity who would absolutely choose to get an abortion with my personal circumstances and where I am in my life, it’s horrifying,” Pliskin said. “Hearing those stories and challenges and people working desperately to overcome them on their own is even more devastating, and sometimes, frankly, traumatizing.”
Sandwiched between Arizona and Texas — collectively home to more than 37 million people and some of the country’s most restrictive abortion laws — New Mexico has administered 232 more abortions each month on average since the Dobbs decision, #WeCount reports.
And since last June, some Planned Parenthood clinics there have seen out-of-state patient loads double — now accounting for 40% of abortions.
Planned Parenthood of the Rocky Mountains President Adrienne Mansanares said they had been anticipating the reversal of Roe v. Wade since former President Donald Trump took office, but “couldn’t have predicted” the impact.
“It’s really important to remember that each of those abortions represents someone’s life and livelihood,” said Ohio State University researcher Mikaela Smith, who is also a member of the #WeCount steering committee.
An emerging “migratory pattern”: Getting to a clinic in the post-Roe era
When Mansanares pulls into the parking lot at work each morning in Denver, she’s greeted by abortion seekers sleeping in their trucks.
Usually, the travelers have Texas license plates.
Dallas to Denver is at least a 12-hour drive. Cities like Austin, Houston and San Antonio are even further.
“It’s like, ‘Oh my gosh, hi, do you need blankets?’ ” Mansanares said. “They’re [like] refugees. They’re seeking care and having to drive through the night to do that.”
One of the couples, she said, drove 17 hours to get there, leaving their cellphones behind for fear of being tracked and criminalized.
“I can’t even drive to my kid’s school without my phone,” Mansanares said. “I can’t imagine driving 17 hours to go to a [clinic you’ve] never been to. … And when they arrive they have no phone. They are so fearful that they are going to be arrested, that they’re doing something wrong.”
About 32,260 fewer Americans received an abortion within six months of the Dobbs decision than before, reports #WeCount. And a study published six months after Dobbs found that the average commute to reach a provider had quadrupled, to about 100 minutes.
Mansanares has seen some patients from as far as Oklahoma and Florida. And the variation in care from state-to-state — coupled with increased wait times — has created a “migratory pattern” of its own where patients are forced to cross multiple state lines to get an abortion within a timely manner.
Texans, for example, often travel to New Mexico for an abortion. But even after a couple of new clinics opened near the state border in recent months, Mansanares said a two-week wait could send some further north to Colorado — where a decade ago, only 11 women from Texas sought an abortion. Last year, that number was 2,345.
“That’s 20 million people who don’t have abortion care in the state they live in,” Mansanares said, noting that wait times used to be three days. “We’re not going to be able to see 20 million people in New Mexico.”
“There’s the next patient, and the next”: Life at the clinic
Because of increased demand for abortions, some clinics are having to put patients with less urgent needs — like those seeking contraceptives — temporarily on hold, sometimes leading to a 28-day wait, Mansanares said.
This, in turn, could lead to more unwanted pregnancies and an even greater number of people looking to get an abortion.
To meet increasing demand and make room for people who need in-person support, Mansanares said clinics have been amping up their telehealth options for family planning and birth control. They have also been expanding their hours and improving benefits for staff whose work takes an emotional toll.
“The trauma comes onto our providers and within our staff as well,” Mansanares said. “And it’s really hard to shake off because there’s the next patient, and the next.”
This piece was republished from the WOUB.